Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
The Quick and Dirty Guide to COVID-19
The Quick and Dirty Guide to COVID-19

The novel coronavirus also called COVID-19, SARS-CoV-2, and simply “the coronavirus,” is a viral disease that originated in Wuhan, China, and was rapidly spread around the world in early 2020. This unit will cover the spread of the coronavirus and how EMS professionals can protect themselves from its spread while still providing effective pre-hospital care. The information in this unit will also act as a primer for patient care in the setting of any respiratory pandemic.
Know Thy Enemy: The Pathophysiology of the Novel Coronavirus
COVID-19 is a viral pathogen that enters cells by attaching to a specific receptor on the cell surface. These receptors are found in large amounts in the lungs, heart, and kidneys. After entering the cell, the virus creates copies of itself and destroys the infected cell. These copies then leave the dead cell and infect other cells in the body. It's just called a coronavirus because corona- means "crown" in Latin, and the spike protein makes the viral envelope look like a crown under microscopy.
The typical emergency presentation of a COVID-19 patient is a patient in respiratory distress: tachypneic, tachycardic, hypoxic, and potentially with altered mental status. Cardiac and renal damage may also occur and lead to alternative presentations.
-
Damage to the cells of the lung leads to large amounts of fluid filling the alveoli throughout the lung. This condition is known as ARDS (Acute Respiratory Distress Syndrome) and results in hypoxia that can only be resolved with positive pressure ventilation.
-
Patients may present with symptoms of congestive heart failure due to the virus attacking the cardiac muscle. This presents with all the symptoms listed above in addition to edema of the lower legs, cool/clammy skin, weak pulses, and slow capillary refill. These patients may present weeks after becoming infected as damage to the cardiac muscle can take a significant amount of time to manifest.
-
Damage to the kidneys is rarely seen in the EMS setting as it generally presents some time after damage to the heart and/or lungs has already hospitalized the patient. By the time renal damage develops, the patient is likely no longer capable of spreading the virus.
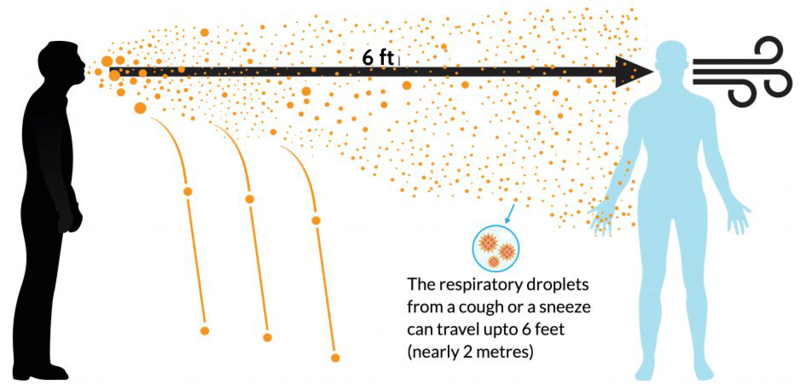
COVID-19 spreads primarily like any cold: through droplets created by talking/coughing/sneezing.
-
COVID-19 is thought to be a “droplet pathogen,” which means that it must be attached to microscopic droplets of saliva or mucus to spread through the air. This differs from an “airborne” pathogen in that droplets are much larger than individual virus particles and can be easily stopped by facemasks. The size of these droplets also helps gravity to pull them out of the air circulation in a room much more rapidly than is seen in airborne pathogens.
-
Fomites are everyday objects that viral particles attach to and can survive on for a significant amount of time. The COVID-19 virus can't survive on a surface for multiple days, but the next accidental release or mutation might. In the early stages of a pandemic, it makes sense to assume that fomites may transmit the disease, and so until we knew it didn't transfer this way, we erred on the side of safety. Some of the most common fomite magnets in the EMS setting are vehicle doors, used masks/gloves, clothing, cellular phones, radios, and computers. Keeping these wiped down and your hands washed often GREATLY reduces the chances of further spread of any fomite transmissible pathology in any season.
-
Aerosolization is the creation of vast numbers of infectious droplets that can bypass certain types of masks and eye protection. Any aerosolized potent pathology would have the highest amount of transmissibility. Normal droplets are relatively large and leave the air in minutes, but aerosols can remain suspended in the air for hours. Coughing and sneezing create small amounts of aerosols, and certain medical procedures such as bag-valve-mask ventilation, CPAP/BiPAP, and intubation can create massive amounts of aerosols. Many of the specific changes in prehospital protocols surrounding the coronavirus are focused on limiting the creation of aerosols.
Scene Safety During a Pandemic

Scene safety is a priority on all calls. You have no idea what some of these people have or where they got it. If an EMS professional is incapacitated or killed, the local healthcare system loses a powerful asset which can lead to further patient deaths if there are not enough caregivers for an escalating number of patients. This section will review the protective measures that should be taken in a pandemic resulting from a droplet-based respiratory disease like Covid-19.
-
Droplets are the primary method by which COVID-19 and most infectious respiratory diseases spread. Wearing a simple surgical mask and basic eye protection lowers the exposure to droplets significantly. These are the most basic elements of PPE that should be used during the COVID-19 pandemic. Due to the rapid spread of COVID-19, it is prudent to treat all patients as if they are infected and utilize basic mouth/nose/eye protection with all patients. The concept of “social distancing” in public spaces is intended to limit droplet transmission of the virus. In the event that a patient is undergoing a procedure that creates a significant number of aerosols, it is recommended to wear a fit-tested N-95 mask. These masks are better able to block small aerosolized particles than a common surgical mask.
-
Fomites are the second most significant way pathology spreads, though not a huge factor in Covid-19. Sterilizing objects such as stretchers, radios, door handles, and clothing is essential to limiting fomite spread. Aggressive use of disposable gloves and frequent hand washing also dramatically lowers the risk of infection by fomites. Adjusting glasses/contacts/masks and eating or drinking without performing full hand hygiene confers a significant risk of infection via fomites and is how the majority of healthcare workers are suspected of becoming infected.
-
The final key to preventing COVID-19 or other coronavirus spread is to limit the opportunities that the virus has to aerosolize. Placing a surgical mask on a patient with an active cough or sneeze is one of the most effective ways to limit aerosolization. There are also several interventions that are known to increase the amount of aerosolization; BiPAP, CPAP, Bag-Valve-Mask ventilation and Intubation have all been shown to create a significant number of aerosols. These interventions should be limited unless absolutely necessary, and local protocols may forbid them in some jurisdictions.
Treatment Changes in the Setting of Suspected Aerosolized Pathogen
The treatment of COVID-19 patients in the prehospital setting is similar to that of any patient with acute respiratory distress, Aggressive control of the ABC’s with a focus on maintaining a patent airway and sufficient ventilation to oxygenate the blood and remove carbon dioxide. COVID-19 limits some effective EMS interventions due to risks to EMS professionals and early evidence showing limited benefit.
-
The most common change in the management of respiratory distress secondary to suspected aerosolized pathology is the relative contraindication to CPAP and BiPAP. Noninvasive modalities of airway support have been shown to have little benefit in improving respiration or ventilation while aerosolizing large numbers of virus particles. If local EMS protocols still call for these treatments to be attempted, a HEPA viral filter should be placed inline between the positive pressure mask and the CPAP/BiPAP device. The same is true when ventilating with a bag valve mask.
-
Early intubation has been shown to improve outcomes in confirmed COVID-19 cases. These intubations need to be done in a manner that minimizes the aerosolization of viral particles. Due to this reason, many jurisdictions will not allow for field intubations in suspected COVID-19 patients. If a patient is beginning to show signs of severe hypoxia (cyanosis, altered mental status, tachycardia) it is reasonable to attempt placing a nasal cannula at 10 LPM and a non-rebreather mask at 15 LPM over the nasal cannula and run both simultaneously.
-
Due to the two above reasons, the airway and oxygenation of suspected COVID-19 patients are best supported by nasal cannula or non-rebreather mask or both. Even in the event of hypoxia, many jurisdictions do not advocate escalating to CPAP or BiPAP unless mental status change develops. Placing patients in the prone position can assist with shortness of breath and low oxygen saturations but should be done with caution in the EMS setting only if local protocols allow for it due to the risk of suffocation and increased difficulty of reassessing the patient.
-
COVID-19 patients are very sensitive to fluid overload, and IV fluids should be used sparingly, even in the setting of hypotension. Small boluses of 250ml are recommended.
-
The transport of suspected COVID-19 patients may be guided by local protocols that direct all suspected COVID-19 cases to a specific hospital or hospital entrance.
Post Shift Safety
 The presence of a pandemic dramatically increases the risk of “bringing your work home with you,” as there will be countless possible and/or confirmed exposures to COVID-19-positive patients and contaminated fomites throughout an average shift. This section will focus on several recommended steps to prevent the spread of COVID-19 between EMS providers and household members.
The presence of a pandemic dramatically increases the risk of “bringing your work home with you,” as there will be countless possible and/or confirmed exposures to COVID-19-positive patients and contaminated fomites throughout an average shift. This section will focus on several recommended steps to prevent the spread of COVID-19 between EMS providers and household members.
-
Upon returning from a shift, the first essential step is to clean all washable equipment to remove fomites, then remove the outer layer of clothing and wash/dry the clothing with soap on the highest heat that the clothing can sustain to kill all viral particles. Facial hair and hair on the head should be washed normally using any shampoo.
-
Shortages of PPE are prompting near-universal recommendations to reuse surgical masks, N-95 masks, and certain gowns/gloves if at all possible. Current recommendations are to discard visibly soiled PPE and don't re-use the same N95 masks day after day. If reusable gloves and coveralls were provided, they are best washed with dish soap and hot water and then hung to dry if specialized disinfecting solutions/machinery is not available.
-
Rules for social distancing and wearing masks in public exist to slow the spread of disease as opposed to preventing its transmission entirely. When out in public in an area that is frequented by large numbers of people, i.e., gas stations, banks, grocery stores, ATMs, restaurants, and stores, it is prudent to practice hand hygiene immediately after leaving the store and before touching any personal objects such as car keys, phones, facemasks, glasses, and car doors. As a healthcare professional, your knowledge of fomites and how to effectively prevent their creation is your strongest defense against infection.
Additional Details
This section will focus on some of the non-EMS relevant details that patients, bystanders, or family members may ask about COVID-19 and some of the newsworthy events surrounding it.
- Social Distancing: The concept of reducing the spread of a virus by limiting contact between individuals in the community is the foundation of the public health response to any pandemic. If you're not surrounded by people, you're not breathing each other's air.
- Prevention and home treatment: A non-sedentary lifestyle with a healthy diet and plenty of morning sunshine is your best shield against all illnesses. If you are deficient in vitamin C, D, or zinc, supplementation may be beneficial.
- When to seek medical care: If you or a loved one develops tachypnea and/or shortness of breath at rest or other signs of hypoxia, they should be brought to the emergency department. Fevers, fingertip pulse oximeters, and tachycardia are unreliable signs of severe illness and are extremely unlikely to require hospitalization or care in the emergency department.
- Vaccines: Initially, people were told that vaccination would protect them from getting the virus and would prevent them from spreading the virus resulting in nearly 70% of the USA getting "fully vaccinated" against the virus. Boosters are available, but as of Nov. 8th, 2023, only about 15% of the US has taken the latest booster.
This is an evolving situation and an evolving guide! Get the best info you can from all trusted sources, follow local medical direction, and use your best judgment towards the highest good of your patient.