Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
QUICK AND DIRTY GUIDE TO WORKING A CARDIAC ARREST
The Quick and Dirty Guide to Working a Cardiac Arrest

Prehospital providers who are not well-versed in cardiac arrest often perceive codes to be difficult. However, with a little practice, they are quite the opposite. In fact, once you become more proficient with the fundamentals, cardiac arrests will be some of the easiest calls that you ever run (except for the paperwork, of course). Today, we're looking at asystole, which means no cardiac electrical activity.
When to Work a Cardiac Arrest
First, do no harm.
Protocols to withhold resuscitation should be based on the determination that there are no obvious signs of life, the injuries are obviously incompatible with life, there is evidence of prolonged arrest, and that there is no organized electrocardiographic activity. If your patient has evidence of rigor mortis in his jaw (usually the first place you will be able to notice it,) then you are doing harm by providing the family false hope, wasting chronologic and material resources, and abusing a corpse.
Studies show that out-of-hospital arrests that are in asystole when ALS arrives have abysmal survival rates. Even when all seems dark, sometimes you win. In the beginning, work under this idea: Even if your current patient does not benefit from your actions, your next patient may benefit from your proficiency. In the beginning, err on the side of working it.
Where to Work a Cardiac Arrest
Work them where you find them. It is extremely rare for any OHCA (out-of-hospital cardiac arrest) patient to survive and be discharged. When this extremely rare thing DOES happen, it is primarily because medics achieved a return of spontaneous circulation (ROSC) on scene, and THEN transported. The risk of the ambulance being involved in an MVC while driving emergency traffic SIGNIFICANTLY outweighs any advantage you may receive in transporting a patient in asystole. You must, of course, follow your local protocols. But, unless required, only transport when you get a spontaneous pulse back.
How to Work a Cardiac Arrest
Let’s break the process down into steps.
Compressions
High-quality compressions are absolutely crucial in ALL types of cardiac arrest, asystole or not. As the paramedic, you will likely be tied up with ALS interventions, which may leave the compressions to a not-so-experienced firefighter, first responder, or bystander. Just remember, push hard, push fast, allow for chest recoil, and keep the interruptions to a minimum. I’m not familiar with all of the flavors of cardiac monitors, but I do know that our Lifepak 15s have built-in metronomes that help keep the compression person on track. Also, remember that if your patient is intubated, you can monitor the effectiveness of compressions by looking at your ETCO2 (end-tidal CO2). When high-quality compressions are being performed, your ETCO2 should be around 10mm/hg.
Defibrillation
You may be saying to yourself, “I thought this was an asystole code...” True, asystole is not a shockable rhythm but weird things happen in the field. I’ve run patients who went from asystole to a weak pulse and an ETCO2 of 40mm/hg after some killer compressions and a little bit of epi. Unlikely, sure, but weird stuff happens. All that to say this: just put the defib pads on and continue your rhythm checks after every cycle of CPR. Do it the right way no matter what you think the outcome might be.
IV Access
If you’re lucky enough to have a medic or IV-certified EMT as a partner then you can delegate this task. If you don’t then you’re the man. Get two if you can but at the very least get one large bore line that is in a sturdy vessel. Go for the EJs and the ACs. If the patient has neither, then utilize an interosseus (IO) needle or drill such as the EZ IO. Access is essential!
Pharmacology
Here is a list of some of the most common drugs used in cardiac arrest. This is by no means all-inclusive but this list covers most of the bases.
- Epi 1:10,000 - 1mg IV given every 3-5 minutes. 2mg can go in the tube. Used primarily for its alpha 1 characteristics to increase afterload and thus increase coronary perfusion. Not shown to consistently improve out-of-hospital survival rate.
- Amiodarone - 300mg, 150mg (2nd dose) given for refractory vfib (vfib that is not responding to defibrillation).
- Sodium Bicarb - 1mEq/kg given after the patient has received high-quality ventilations, preferably with an advanced airway. If you do not have a way to provide high-quality ventilations then you will put your patient into a very severe respiratory acidosis. Epi can be empirically given to dialysis patients.
- Narcan - 2mg+ for patients who have overdosed on opioids.
Airway
Airway has taken a bit of a back seat ever since the new ACLS guidelines came out but it is still vital in the proper management of a cardiac arrest. Ultimately, endotracheal intubation is the end all be all mode of airway management. Not only does it provide you with the best ventilations and the most accurate ETCO2 but it also offers complete airway protection. Your efforts may be all for naught if your patient aspirates during the code. Alternatively, there are supraglottic airways such as the King or i-gel. Both are extremely easy to place and come in handy when you come across a patient that you’re unable to intubate.
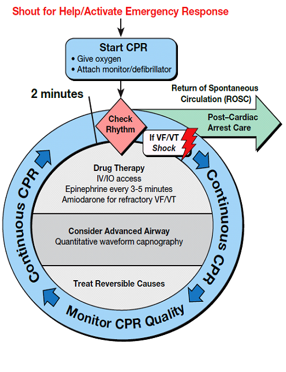
A rough step-by-step guide outlining each of the major goals of running a code
- Assess the patient for a pulse - Check a carotid pulse and look to see if the patient is breathing.
- Begin compressions - If the patient is apneic and pulseless, have your partner hop on compressions.
- Attach the monitor - Attach those pads and switch your monitor to paddle mode. This will allow you to view the patient’s rhythm (or lack thereof) through the pads.
- Check the rhythm - In the case of an asystole arrest, you will not defibrillate. But, if the patient does convert to a shockable rhythm such as vfib or vtach without a pulse then you may defibrillate at 200J biphasic.
- Get into your compressions cycle - Compressions 2 minutes at a time with rhythm checks in between. Ventilate twice after every 30 compressions until you get an airway.
- Start your IV and give your drugs - Grab that line, get fluids going wide open, and start the epi cycle. Consult the ACLS algorithm for when to give your other drugs.
- Obtain your airway - Tube the guy if you can, King or iGel him if you can’t. Regardless, try to move to an airway that allows you to ventilate asynchronously. Once this is done, breathe once every 6 seconds and watch that ETCO2!
- Rinse and repeat - That’s just about it. Settle into this cycle and reassess your patient regularly. You also need to be considering your 12 reversible causes and taking the steps to correct them.
H's and T's
The H’s and T’s of ACLS is a mnemonic used to help remember the major causes of pulseless arrest including PEA, Asystole, Ventricular Fibrillation, and Ventricular Tachycardia. These H’s and T’s are most commonly appropriate for PEA, but you may be questioned about them during class or your National Registry Practical Exam for any ACLS algorithm.
The H’s
Hypovolemia - Insufficient blood volume
Hypoxia - insufficient oxygenation
Hydrogen ion - acidosis
Hyper-/hypokalemia
Hypothermia - insufficient heat
Hypo-/Hyperglycemia - Blood sugar too low or too high
The T’s
Toxins - ingestions
Tamponade - cardiac
Tension pneumothorax
Thrombosis - pulmonary and cardiac
Trauma
Thromboembolism (PE)
When to Stop Working a Cardiac Arrest
Best said by Navarro on EMS1
The latest American Heart Association (AHA) Guidelines recommend two different strategies for field termination of resuscitation efforts (Morrison et al., 2010). For exclusively BLS systems, EMS personnel should consider field termination when three termination criteria exist: (a) no EMS professional witnessed the onset of arrest; (b) no ROSC after three full rounds of CPR and AED analysis; and (c) no shock delivered by the AED.
For ALS systems, the AHA recommends that advanced-level providers consider field termination when four criteria exist: (a) no one witnessed the onset of the arrest; (b) no bystanders performed CPR prior to EMS arrival; (c) the patient never achieved ROSC after full ALS implementation; and (d) no shock delivered by an AED. In October 2011, the National Association of EMS Physicians (2011) issued a position paper on field termination of resuscitation efforts stating that EMS personnel should consider field termination when three criteria exist: (a) no EMS professional witnessed the onset of the arrest; (b) there was never a shockable rhythm present; and (c) the patient never achieved ROSC on scene.
Editor's Note: I believe that the skill and algorithm of working a cardiac arrest should come FIRST in EMT/Paramedic school. This is a repeatable skill that should be taught early and repeated often. At first you will know WHAT to do, and over the course of your schooling and your career, you will learn WHY to do each part. Untold amounts of students are still trying to memorize this algorithm at test time. This is primarily because most Paramedic Schools wait until the last semester before learning ACLS. This is a skill, and you must practice it often in scenarios and theoretical environments. This way, you're not reaching for a book when this call comes out at 1am and you're doing it live in front of a real family who needs you to know what you're doing.