Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Pneumonia
Category: Airway
Topic: Respiratory Ilnesses and Disease
Level: Paramedic
Next Unit: Chronic Obstructive Lung Diseases for the AEMT
14 minute read
Pneumonia
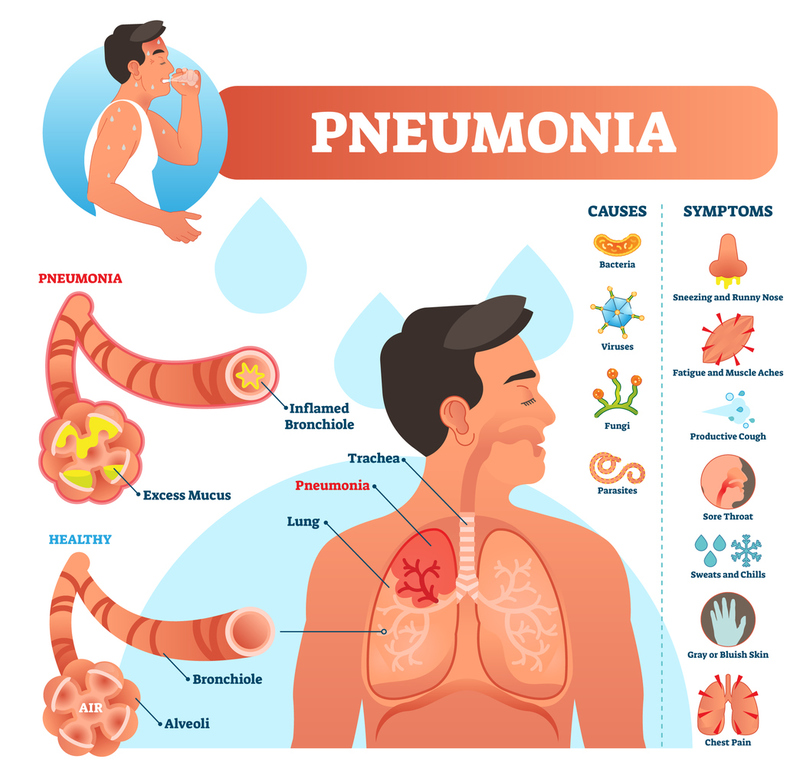
Pneumonia is a common condition that leads to many EMS calls, it often begins similarly to a generic cold or flu; gradually developing into a severe set of pulmonary and systemic symptoms that often lead the patient of loved ones to contact EMS. This section will review some of the definitions, subtypes, signs/symptoms, and management specific to pneumonia.
Definitions
PNEUMONITIS: inflammation of the lungs.
PNEUMONIA: inflammation of the air sacs (alveoli), with the added feature of pulmonary consolidation (filling of the alveoli with fluid).
Classifications
Pneumonia can be classified by how/where it is acquired, by the infecting agent, or anatomically.
1) ACQUISITION
- Community-acquired pneumonia (CAP): "standard" pneumonia, commonly used to refer to pneumonia in patients who have not been recently exposed to healthcare environments.
- Hospital-acquired pneumonia (HAP): also called nosocomial pneumonia, refers to lung infections in patients who have been exposed to hospitals, nursing homes, or emergency rooms in the past 90 days. The classification is important because the organisms involved in this class of pneumonia is often multi-drug resistant.
- Aspiration pneumonia (AP): accidental introduction of bacteria into the lungs when food, drink, vomit, or saliva is inhaled into the airway. This generally occurs in patients with disturbances in their gag reflex, brain injuries, or excessive use of substances.
- Organizing pneumonia: a broad group of conditions with similar symptoms caused by the chronic inhalation of certain dusts, chemicals, or proteins. Sometimes called pneumoconiosis.
2) INFECTING AGENT
- Bacterial pneumonia: Often spontaneously develops as a bacterial complication following a cold or the flu. More common in patients older than adolescence and generally considered more severe than viral pneumonia.
- The most common cause of bacterial pneumonia is Streptococcus pneumoniae.
- Viral pneumonia: Arises when the same viruses that cause simple colds and the flu manages to infect the lower respiratory tract. Most common in children under 5 years of age. While usually mild and less severe than bacterial pneumonia, viral infections can still become very serious.
- Atypical pneumonia: also called Mycoplasma Pneumonia and "Walking Pneumonia," It is caused by a large number of strange and atypical bacteria, hence the name. The infection is generally very mild and rarely leads to emergency activation unless the patient is immunocompromised (cancer, HIV, genetic issues, ect.).
- Fungal pneumonia: Common in certain geographic areas, fungi that cause disease can be present in the soil, bird droppings, and on certain wild animals. Repeated or severe fungal infections are often a sign of immunocompromise as the human immune system can generally fight off these infections easily.
3) ANATOMY
- Lobar pneumonia: involvement of a single lobe or a segment of a lobe.
- Bronchopneumonia: primary involvement of the larger airways and surrounding tissue.
- Necrotizing pneumonia: the destruction of large amounts of lung tissue, generally associated with aspiration.
- Caseating granuloma: seen with pneumonia due to tuberculosis, exceptionally rare in the United States.
- Interstitial pneumonia: affects the alveolar walls and the tissue that makes up the lung more than the small airways that lead to the alveoli, these types of pneumonia present with atypical symptoms and can be unresponsive to typical oxygenation/ventilation strategies.
Signs and Symptoms
The signs and symptoms of pneumonia center around the lungs in patients with mild disease and the whole body in patients with severe disease.
MILD DISEASE: The symptoms of mild pneumonia are generally limited to fever, cough, shortness of breath (dyspnea), and chest pain. The signs often include tachycardia, tachypnea, and abnormal lung sounds. The lung sounds in pneumonia are referred to as "crackles" and "consolidation."
Crackles, described as "velcro pulling apart" or "popcorn sounds" are caused by alveoli that are filled with fluid popping open as a patient takes a breath.
Consolidation is the increased volume of sound over an area that is filled with fluid. This occurs because sound travels more easily through a lung whose alveoli are filled with pus/blood/edema, such as in pneumonia. A key finding on lung examination is the presence of bronchial breath sounds—harsh, tubular sounds that are normally heard over the trachea but become abnormally audible in the outer areas of the lungs when consolidation is present.
SEVERE DISEASE: Severe pneumonia has all the above-mentioned signs and symptoms with a few special extras. Patients with severe disease may experience chills, sweating, flushing of the skin, and confusion. Vital signs are often more severely deranged, with low SPO2 and low/high end-tidal CO2 (outside 35% to 45%) joining the expected tachycardia and tachypnea.
Sepsis is a common result of severe pneumonia, watch carefully for dropping blood pressure and changing mental status!
Management
Managing pneumonia always revolves around airway and breathing, in severe cases with sepsis circulation also becomes a concern. Regardless of the severity, regular reassessment is key, declining SPO2 or changing mental status demands attention!
MILD PNEUMONIA: EMS may be contacted for patients with mild pneumonia if they reside in nursing homes or have other medical conditions that worry family members. These patients will generally only require mild oxygen if anything at all. Focus on rapid transport and watching for signs of more severe disease such as dropping blood pressure, dropping oxygenation, or increased heart rate/respiratory rate.
SEVERE PNEUMONIA: Severe illness leads to many more EMS calls than mild illness. These patients may be in an unstable condition, requiring positive pressure ventilation and close monitoring of SPO2, end-tidal CO2, and blood pressure. Place large bore IV's in these patients and re-assess extremely frequently for the development of sepsis.
Keep in mind that providing oxygen in patients with chronic respiratory illness such as COPD/Emphysema can lead to respiratory arrest, be prepared to provide positive pressure ventilation! This phenomenon is explained further in the COPD section.