Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Meningitis
Category: Medical
Topic: Infectious Diseases
Level: Paramedic
Next Unit: Tuberculosis
14 minute read
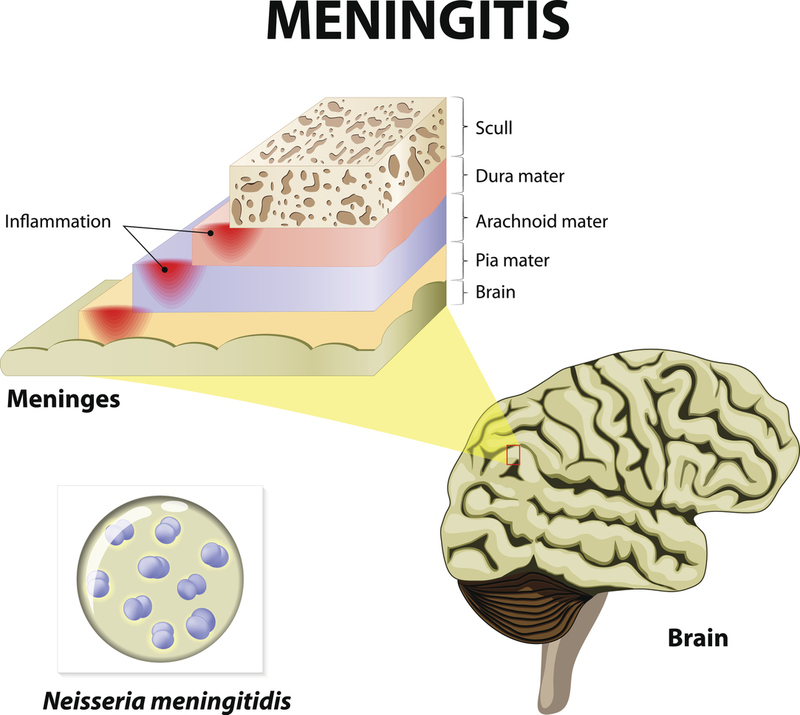
The brain is wrapped in three protective layers called meninges.
MENINGITIS: Meningitis is an inflammatory disease of the tissues surrounding the brain and spinal cord. Primarily, the leptomeninges!
LEPTOMENINGES: The inner two meninges, the ARACHNOID and the PIA MATER, between which circulates the cerebrospinal fluid. The infection is active in this moat.
(The outermost layer of the three meninges is the dura mater.)
ENCEPHALITIS: Infection of brain tissue, accompanied by neurologic dysfunction. It is considered a progression from meningitis (meningoencephalitis).
►The presence or absence of normal brain function is the important distinguishing feature between encephalitis and meningitis.
Patients with meningitis may be lethargic or distracted by a headache, but their cerebral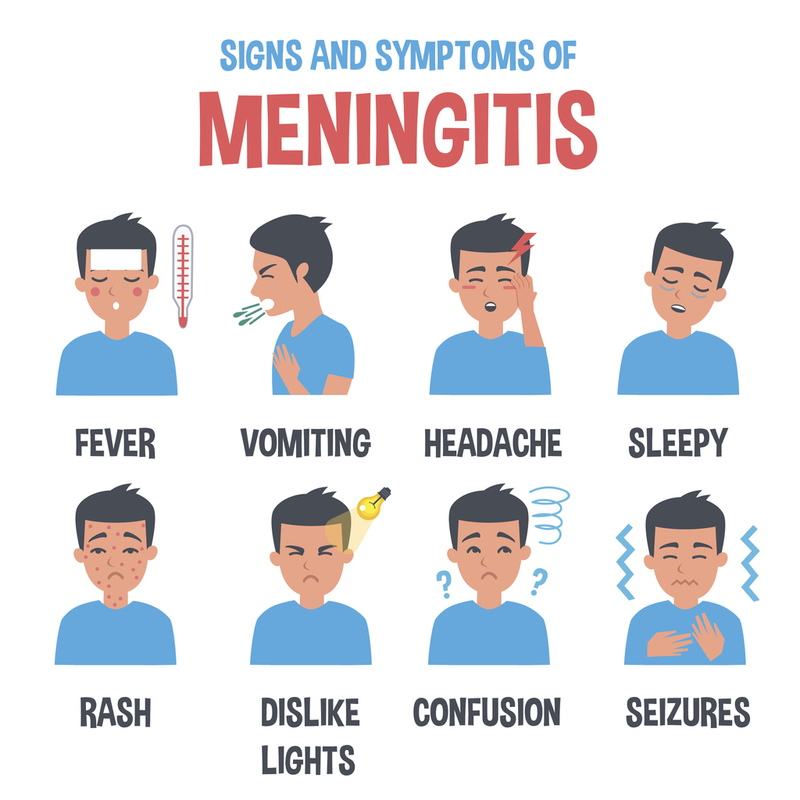 function remains normal. In contrast, patients with encephalitis commonly present with abnormalities in brain function, such as
function remains normal. In contrast, patients with encephalitis commonly present with abnormalities in brain function, such as
- altered mental status,
- motor or sensory deficits,
- altered behavior and personality changes, and
- speech or movement disorders.
Clinically, however, there can be a blurring of these two distinctions.
CAUSE: Meningitis is thought to develop from invading organisms from the nasopharynx, from bacteremia (such as in infective endocarditis), or due to direct entry into the central nervous system from spillage of infectious fluids/material from sinuses, via trauma, or with implanted medical devices.
COMPLICATIONS: Complications from meningitis, meningoencephalitis, and encephalitis include seizures, cerebral edema, cardiorespiratory failure, coma, and death.
Types of Meningitis
VIRAL MENINGITIS: a febrile illness with clinical signs and symptoms of meningeal irritation and no evidence of bacterial pathogens in the CSF. It is most commonly due to
- Enteroviruses (85-95% of cases) via a fecal-oral route.
BACTERIAL MENINGITIS: meningeal inflammation due to bacterial infection. It can be either community-acquired or healthcare-associated. It is most commonly due to
- Streptococcus penumoniae
- Neisseria meningitidis
- Listeria monocytogenes (commonly in those over 50)
NOTE: Patients with bacterial meningitis are usually quite ill and often present soon after symptom onset (usually less than 24 hours). Viral meningitis is usually a milder illness.
ASEPTIC MENINGITIS: This is clinical and laboratory evidence for meningeal inflammation with
- negative routine bacterial cultures and usually has
- no neurologic dysfunction.
This does not mean no organisms have caused it; on the contrary, most commonly, it is due to enterovirus.
In fact, many use the terms aseptic meningitis and viral meningitis synonymously.
Aseptic meningitis can also be caused by:
- mycobacteria,
- fungi,
- spirochetes (syphilis),
- medications, or
- malignancy.
NOTE: In bacterial meningitis, the CSF will exhibit an elevation in WBCs and protein, but a drop in glucose from normal values. In viral meningitis, there will be lower concentration (even normal) of WBCs and protein, a normal CSF glucose, and negative CSF bacterial cultures. Sometimes a subsequent spinal tap is needed to identify a shift in findings.
Signs and Symptoms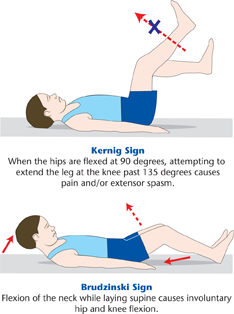
THE CLASSIC TRIAD:
- Fever (in 95% of patients)
- Nuchal (neck) rigidity (88%)
- Mental status changes (indicative of overlapping encephalitis) (78%)
(One or more of these may be absent, but 99% of meningitis patients have at least one of these three findings.)
OTHER S&S:
- Headache
- Seizures
- Focal neurologic deficits, such as cranial nerve palsies
- Nausea and vomiting (and, in children, subsequent dehydration)
- Hearing loss
- Skin rash-type changes, notably petechiae, and purpura, particularly with N. meningitidis, whose bacteremia causes thrombocytopenia (low platelets).
- Arthritis
Kernig's sign is a clinical sign used to diagnose meningitis.
Here's how the test for Kernig's sign is performed:
The patient is first placed supine (lying flat on the back).
The medical professional then bends the patient's hip and knee at a 90-degree angle.
After this, the professional attempts to straighten the patient's leg at the knee.
Kernig's sign is considered positive if the patient experiences pain and resistance during the leg extension, often causing the patient to bend the knee involuntarily. The pain is due to the stretching of the inflamed meninges and is a suggestive sign of meningitis. However, Kernig's sign is not always present in people with meningitis and may also be present in other conditions, so it isn't 100% reliable on its own for diagnosis.
Brudzinski's sign is another clinical sign used in the diagnosis of meningitis. It's performed as follows:
The patient is placed in a supine position (lying flat on the back).
The medical professional then gently lifts the patient's head, causing the neck to flex towards the chest.
Brudzinski's sign is considered positive if this maneuver causes the patient's knees and hips to flex involuntarily. This happens because the action of lifting the head stretches the inflamed meninges, leading to discomfort and the reflex action.
Like Kernig's sign, a positive Brudzinski's sign indicates meningitis, but it is not entirely reliable on its own. Some meningitis patients may not display a positive Brudzinski's sign, which can also be positive in other conditions. Additional testing, such as a lumbar puncture, is necessary for a definitive diagnosis of meningitis.
Management
The most important factor is determining whether meningitis is viral or bacterial because administering antibiotics can be life-saving when it is found to be bacterial. Since this is determined via lumbar puncture (spinal tap), you, as an EMS responder, will not be required to make that distinction. Your big responsibility is recognizing the LIKELIHOOD of meningitis and supporting the patient en route.