Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Drugs of Abuse and Medication Overdose
Drugs of Abuse and Medication Overdose

15% of all people have a genetic predisposition to addiction. It need not be drugs or alcohol; it can be gambling, over-eating, dieting, exercise, pornography, or even religious fanaticism. Just because someone has a predisposition does not mean addiction to something is guaranteed. Many people reason through these tendencies via fear of incarceration, losing their job, jeopardizing their relationship, losing their moral compass, or losing self-esteem.
Definitions
DEPENDENCE: if one feels physical and/or emotional symptoms of withdrawal when stopping the medication or substance.
WITHDRAWAL: the actual physical and emotional discomfort when stopping a medication.
TOLERANCE: when it takes more of the medication or substance to achieve the same result as previously.
CROSS-TOLERANCE: when tolerance to the effects of one drug causes tolerance to another drug, often between drugs with similar functions or effects.
ADDICTION: when dependence is so strong physically or emotionally that one would indulge in maladaptive behavior to get it, including lying, stealing, or worse.
PSEUDO-ADDICTION: when persons watch the clock in anticipation of their next dose, uncomfortable due to pain relief, as prescribed, failing before the next dose is due. This has nothing to do with addiction but indicates a condition of pain is being under-treated.
Drugs of Abuse
While all drugs have the potential to be "abused" the prevalence and consequences of abuse vary heavily from drug to drug. Generally, you can divide drug abuse into "social" drugs and "medical" drugs of abuse, keep in mind that there is quite a bit of crossover between the two.
Social Drugs of Abuse: Social drugs are those such as alcohol, opiates (heroin), cannabis, hallucinogens (party drugs), stimulants (cocaine/methamphetamine), and inhalants. Some of these drugs are legal and regulated, while others are acquired from suspect sources and may be contaminated.
Medical Drugs of Abuse: Medical drugs such as opiate pain medication, stimulants (Adderall), depressants, and cholinergic/anticholinergic medications can all be abused both by those they are prescribed to and those that acquire them illicitly. The nature of the abuse can be excess use for their intended purpose or use for an entirely unintended purpose.
Opiates/Narcotics
COMMON CAUSES: Opiate and narcotic abuse most commonly result from past injuries that have resulted in heavy pain medication use and a resulting dependence that was never broken. A smaller number of patients become addicted through experimentation and/or seeking to escape from the mental and physical pain of depression, anxiety, abuse, or peer pressure.
COMMON SUBSTANCES: While injectable forms (heroin, morphine, fentanyl) are the most dramatic and have a greater risk of non-overdose complications. Oral forms (codeine, methadone, hydrocodone, oxycodone) and transdermal forms (fentanyl) can be just as deadly in overdose as an injection.
ASSESSMENT FINDINGS and symptoms consistent with opiate/narcotic abuse include altered mental status, pinpoint pupils, nausea/vomiting, hypotension, respiratory depression, seizures, and coma.
TREATMENT: The long-acting opioid agonist methadone is commonly used to eliminate withdrawal symptoms and to provide a means for weaning. The mortality rate of withdrawal is very low, although it is insufferably uncomfortable. Also, see naloxone below.
MANAGEMENT of patients with suspected narcotic/opiate abuse/narcosis focuses around maintaining the airway and breathing.
Respiratory depression is often what leads to death in acute overdose, the body loses the ability to increase the respiratory rate in response to low oxygenation, resulting in hypoxemic cardiac arrest. Aspiration of vomit due to the inability to protect the airway and brain damage due to hypoxemia are other long-term complications of overdose.
The administration of naloxone, an opioid antagonist, will begin reversing these effects within minutes. Until then, administration of oxygen via bag-valve-mask with the assistance of an airway adjunct and protecting the airway from aspiration (through positioning or placement of an advanced airway) are paramount.
Alcohol
Alcoholism in the EMS setting refers to the state of physical dependence that can result in severe injury or death if consumption is suddenly stopped. Unlike opiates, alcohol withdrawal can be fatal if untreated and is uncomfortable and agitating even if not lethal.
COMMON CAUSES: As with opiates, multiple behavioral and societal factors play into the overconsumption of alcohol. Alcohol abuse is defined as excessive use (acute or chronic) that increases the risk of acute injury or chronic medical issues. While alcohol dependence is a state of physiological addiction that will result in symptoms if use is discontinued.
ASSESSMENT FINDINGS: Acute intoxication with alcohol presents with LOC changes ranging from agitation to sedation, respiratory depression, loss of coordination, and nausea/vomiting. Chronic use can also have detrimental health effects that may appear on the exam, including malnutrition, pancreatitis, liver disease, head/neck cancer, and neurological damage.
Alcohol withdrawal may begin to occur as soon as 12 hours after the last drink and generally presents with sweating, weakness, and tremors, potentially developing into seizures, and in severe cases, hallucinations and autonomic instability (tachycardia, wild BP swings, alterations in respiratory rate). As mentioned above, severe withdrawal is a medical emergency.
MANAGEMENT As a mild anesthetic, ethanol can reduce the patient's perception of pain. It is important to carefully and completely examine the patient for any unnoticed injuries.
Management of patients with suspected alcohol abuse or withdrawal is again focused on the ABC's keeping the airway patent with adjuncts if necessary and clear of any debris. Ensuring the respiratory rate is adequate and the risk of aspiration is minimized, and checking circulation in patients with severe withdrawal.
Medical command may authorize the use of IV benzodiazepines in patients who are showing signs of severe withdrawal (seizure/hallucination), these medications may also help to calm patients that may become agitated in transport.
Cannabis
COMMON CAUSES: cannabis abuse includes peer pressure, depression/anxiety, and a gradual increase in the frequency of recreational use. Cannabis use is considered abuse when it impairs a patient's typical patterns of social functioning.
ASSESSMENT FINDINGS: Acute cannabis use can present with distorted perceptions, impaired coordination, difficulty with problem-solving, and problems with learning or memory. Relatively benign symptoms such as cough, red eyes, hunger, and dry mouth are common. More serious side effects such as nausea/vomiting, tachycardia, anxiety, paranoia, and loss of physical control can lead to harm.
MANAGEMENT of patients with suspected cannabis use generally revolves around emotional support, transport is rarely required, and life threats are rarely present. Transport may be indicated if extreme paranoia, anxiety, or fear leads to the patient becoming a danger to themselves or others.
If severe symptoms that affect the airway, breathing, or circulation develop, consider the possibility of a second drug being used in conjunction with cannabis!
Hallucinogens
Hallucinogens are a broad category of drugs with many mechanisms of action. Unlike other drugs, addiction to hallucinogens is rare, but acute use can have dramatic effects that are not seen with other drugs. This section will review hallucinogens as a category, with less emphasis on individual drugs.
COMMON CAUSES of hallucinogen use are specific social events (raves, parties, etc.) and anxiety/depression. These drugs are often used concurrently with alcohol and cannabis, potentially increasing their effects and side effects.
COMMON SUBSTANCES in the hallucinogen category include Psilocybin (shrooms), Peyote, jimson weed, mescaline, and LSD. Phencyclidine (PCP) is a hallucinogen that also has significant stimulant effects and a unique set of symptoms.
ASSESSMENT FINDINGS The hallmark symptoms of hallucinogens are visual and auditory hallucinations that result in loss of contact with or an altered perception of reality. This commonly results in a poor perception of time, poor judgment, risky behavior, and confusion. Extremes of emotion with significant anxiety, agitation, panic, fear, or terror may also result.
Physiological symptoms such as dilated pupils, hypertension, tachycardia, hyperthermia, diaphoresis, dizziness, dry mouth, and insomnia may also result.
Countless other symptoms can also result from the mixers used to bind the drugs into tablets or dilute them.
The drug PCP is notable for inducing extreme aggression, agitation, physical strength, and resistance to pain. These patients can be immensely dangerous and often require law enforcement assistance.
MANAGEMENT of patients with suspected hallucinogen use focuses around keeping them calm, ensuring the scene is as quiet as possible and minimizing the number of providers and physical interventions is ideal. If behavioral complications develop, do not hesitate to contact law enforcement to maintain scene safety.
Keep the ABCs in mind if complications develop, patients may require oxygen support for anxiety or medications to reduce blood pressure and heart rate. In rare cases, airway management may be needed if a patient falls unconscious or vomits.
SAFETY FIRST: Don't hesitate to use restraints if there is any danger to the patient, other persons, you, or your team.
Stimulants
Stimulants differ from the aftermentioned drugs in that they primarily provoke increases in energy, focus, and aggression with potential increases in anxiety, fear, and risk-taking.
COMMON CAUSES of stimulant use are similar to hallucinogens, they are often party drugs used by those in young adulthood. Unlike hallucinogens, stimulants also see chronic use in non-social environments as they form a much stronger physiological dependence (addiction).
COMMON SUBSTANCES By far, cocaine, methamphetamine, and medical stimulants for ADHD (Adderall, Vyvanse) are the most common stimulants that are used and abused.
ASSESSMENT FINDINGS and symptoms associated with use include behavioral changes such as euphoria, aggression, agitation, poor sleep, and risk-taking behavior.
COCAINE: Dilated pupils, hyperactivity, tachycardia, diaphoresis, and nausea reflecting stimulation of the sympathetic nervous system, are classic signs of cocaine use.
METHAMPHETAMINE: Life-threatening intoxication with methamphetamine will present with sympathomimetic stimulation: severe agitation, delirium, seizure, hypertension, tachycardia, hyperthermia, and metabolic acidosis. "Meth Mouth": tooth decay is common with chronic abuse due to decreased saliva and bruxism.
Physiological symptoms include tachycardia and hypertension, potentially to dangerous degrees, especially in older patients. Tremors, seizures, nausea/vomiting, shortness of breath, and dangerous increases in body temperature are also seen with stimulant use.
MANAGEMENT of patients with suspected stimulant use is focused on keeping the patient calm and treating the sympathetic overactivation if it is causing significant symptoms, circulation is the most common element of the ABCs compromised by stimulant use. Providing oxygen may minimize anxiety and shortness of breath, and agents to reduce blood pressure and heart rate may be required in extreme cases.
Depressants: Barbiturates/Sedatives/Hypnotics
While other drugs (alcohol) are considered depressants, sedatives and hypnotics are given their own category due to their ability to cause dangerous symptoms in much lower doses. They are some of the most commonly abused drugs behind alcohol and opiates.
COMMON AGENTS The most common sedative that is overused/abused are benzodiazepines (benzos) they come in many forms, the most commonly abused being Xanax, Valium, and Clonazepam. More extreme sedative abusers may use drugs such as barbiturates or other agents normally used for surgical operations.
COMMON CAUSES of sedative/hypnotic use are over-prescription for anxiety and insomnia. They are also commonly used alongside alcohol as a party drug.
ASSESSMENT FINDINGS and symptoms associated with abuse of sedative/hypnotics are drowsiness, apparent intoxication (slurred speech, confusion, disinhibition, and poor coordination). Some patients may have a paradoxical reaction and exhibit aggression, agitation, and risk-taking behavior.
Extreme doses of sedatives can result in dramatic respiratory depression, inability to protect the airway, coma, and resulting death. The combination of small doses of sedatives with alcohol can also result in these deadly symptoms in relatively low doses.
MANAGEMENT patients with a suspected use or abuse of sedatives/hypnotics focus on maintaining the airway and ensuring adequate breathing. Respiratory depression is what acutely kills patients using sedatives, and the risk of aspiration from an unprotected airway is a risk factor for complications later down the road.
Circulation is rarely significantly affected by sedative use, in extreme doses the blood pressure or heart rate may be lowered, requiring fluid/pressure support.
Medication Overdose of Legitimate Medicines
COMMON CAUSES of medication overdoses in patients that are prescribed and normally correctly use their medications generally revolves around mistaking one medication for another or becoming confused about when doses were taken. This is most common in the elderly where poor organization of medications, multiple prescriptions (polypharmacy), and poor memory are more prevalent.
COMMON MEDICATIONS IN OVERDOSE include cardiac medications, psychiatric medications, and non-prescription pain medications (aspirin/Tylenol/NSAIDs)
ASSESSMENT FINDINGS and symptoms associated with medication overdoses often include changes in mental status, abdominal pain, nausea/vomiting/diarrhea, abnormal heart rate/blood pressure, and loss of consciousness. These symptoms depend heavily on the nature of and amount of medication taken.
MANAGEMENT of patients with suspected medication overdose is focused on identifying the medication taken and contacting poison control. Medical command and poison control may recommend specific antidotes for certain overdoses. In all cases maintain airway, breathing, and circulation to the best of your ability.
Other Types of Poisoning
HUFFING: Common causes of huffing poisoning include peer pressure, financial problems, and other drug use. Substances used or abused may include air freshener, gasoline, glue, paint, and others.
ASSESSMENT FINDINGS and symptoms associated with huffing poisoning may include
- cardiovascular collapse and ventricular arrhythmias,
- seizures
- Swelling of the mucous membranes in the mouth/nose
- psychosis.
MANAGEMENT of patients with exposure to or abuse of huffing agents includes
- airway and ventilation and circulation,
- pharmacological sedation and restraint, and
- non-pharmacological interventions.
CHOLINERGICS: Common causes of cholinergic poisonings include pesticide poisoning from farming operations and certain manufacturing facilities as well as nerve agents (Sarin, Soman). These organophosphates inactivate acetylcholinesterase and acetylcholine--the parasympathetic neurotransmitter--accumulates, causing overstimulation of muscarinic and nicotinic receptors. (Clinical effects are manifested via activation of the autonomic and central nervous systems and at nicotinic receptors on skeletal muscle--see below.)
ASSESSMENT FINDINGS: Cholinergic poisoning has a specific set of signs and symptoms regardless of the agent that caused the poisoning. This is known as the cholinergic "toxidrome" and results from the toxin affecting the muscarinic receptors in the brain, airways, and on the muscles.
Cholinergic toxins cause parasympathetic overactivation. This leads to SLUDGE Syndrome in low to moderate doses.
- Salivation,
- Lacrimation,
- Urination,
- Defecation,
- Gastric Emesis
SLUDGE syndrome refers to the outwardly visible signs of a cholinergic toxidrome that are easy to separate from other poisonings. There are a wide variety of other signs and symptoms as well. Bradycardia, shortness of breath, wheezing (due to bronchospasm), pinpoint pupils, cyanosis of the fingers, headache, weakness, anxiety, and skin reddening are all common.
MANAGEMENT of patients with suspected pesticide poisoning is focused on identifying the toxin, contacting poison control, avoiding exposure to the toxin while decontaminating the patient, and maintaining the airway/breathing in the face of massive bronchospasm, increased bronchial mucus production, and potential paralysis of the respiratory muscles.
It is often necessary to administer atropine, this can be done via IM autoinjector or via IV, the exact dose and route should be confirmed with poison control as atropine has significant potential side effects. Supporting respiration with oxygen and the airway via endotracheal intubation may be required.
ANTICHOLINERGICS: Common causes of anticholinergic poisonings include
- atropine (used for bradycardia arrhythmias),
- antihistamines (e.g., diphenhydramine),
- sleep aids (e.g., doxylamine),
- scopolamine, and
- tricyclic antidepressants.
ASSESSMENT FINDINGS and symptoms of anticholinergic poisoning all relate to the blockade of the parasympathetic nervous system induced by these medications. The key symptoms of flushed skin, anhydrosis, dilated pupils, delirium, memory loss, seizures, and urinary retention are remembered with the following common sayings.
- "Red as a beet" – Cutaneous vasodilation to compensate for the loss of sweat production.
- "Dry as a bone" (anhidrosis) – Dry skin.
- "Hot as a hare" (anhidrotic hyperthermia).
- "Blind as a bat" (nonreactive mydriasis--pupil dilation) causing blurry vision.
- "Mad as a hatter" (delirium; hallucinations, anxiety, agitation, confusion, hallucinations, bizarre behavior, delirium, psychosis, paranoia, coma, and seizures. Hallucinations typically make people appear to become larger and smaller.
- "Full as a flask" – Decreased desire to urinate and "sphincter-lock."
The earliest objective sign is often a wide complex tachycardia, this is relatively specific as most other drugs that induce tachycardia result in a narrow complex "sinus" tachycardia.
MANAGEMENT for a patient with suspected exposure to anticholinergics is focused on the management of circulation; placing continuous cardiac monitoring and pulse oximetry is vital. Airway and breathing may become compromised if the patient falls unconscious due to a circulation issue, or vomits due to an ingested substance.
The medication sodium bicarbonate is often administered if QRS widening is seen, this helps to stabilize the cardiac system and prevent potentially fatal arrhythmia.
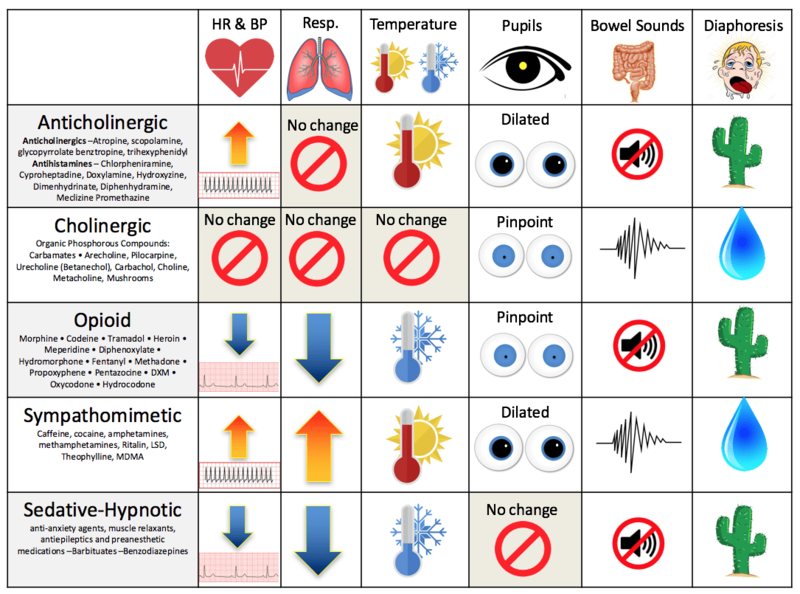
HANDY-DANDY CHEATSHEET OF CHOLINERGIC VS ANTICHOLINERGIC TOXICITY:
CHOLINERGIC: miosis (pupil constriction), sweaty (diaphoresis), and bradycardia or arrhythmias, including heart block and QTc prolongation.
ANTICHOLINERGIC: mydriasis (pupil dilation), dry, and wide-complex tachycardia.
BOTH: agitation.
Remember:
♦ SYMPATHOMIMETIC → PUPIL DILATION (MYDRIASIS)
♦ PARASYMPATHOMIMETIC → PUPIL CONSTRICTION (MIOSIS)