Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Blood Types and Antigens
Category: Medical
Topic: Immunology
Level: Paramedic
Next Unit: Immune Function and Immune Response in Special Populations
16 minute read
The surface of red blood cells (RBCs) are coated with antigens made up of sugars and proteins. These surface molecules can incite an immune response if mixed with red blood cells of a different antigen. Blood (specifically, RBCs) contains antigens that are only compatible with other certain antigens—this is why blood types must be carefully matched for blood transfusions and transplants.
ABO and Rh group systems define one's blood type.
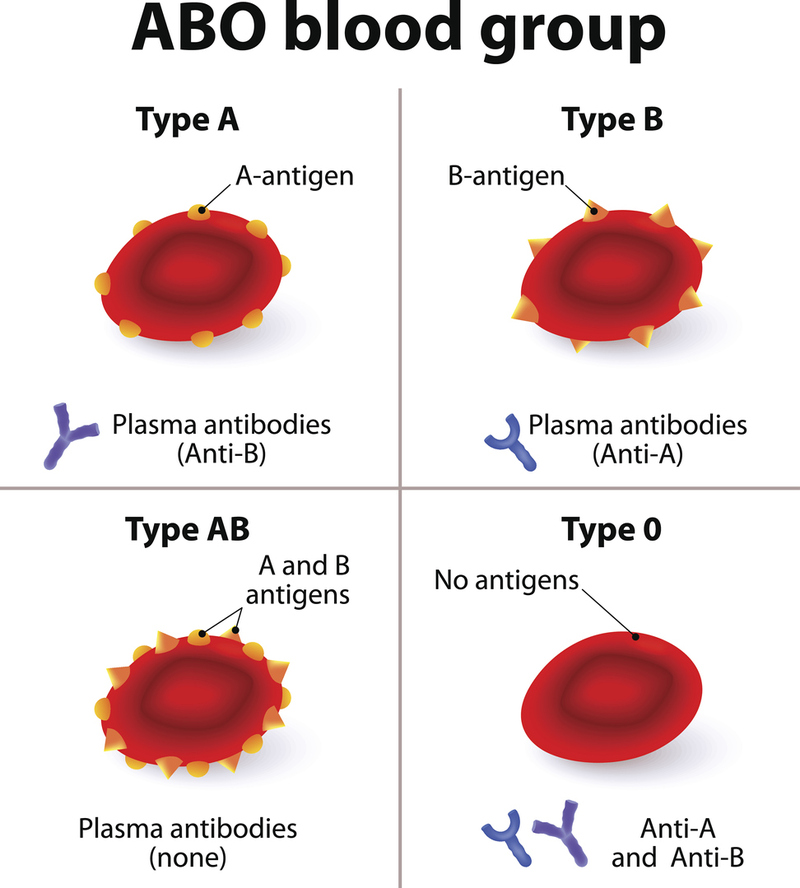
The ABO System
The distribution of the 4 major red blood cell types varies by ethnicity.
Types:
- O,
- A,
- B, and
- AB.
The "A" and "B" phenotypes are distinguishable by their specific sugars.
RBCs have antibodies to the RBC cell types that they aren't:
- Group A individuals will have anti-B antibodies
- Group B individuals will have anti-A antibodies
- Group O individuals will have both anti-A and anti-B antibodies
People with type-O blood are called universal donors because their blood can be given to people with any of the ABO blood types. (Actually, they need to be Rh-, too, to truly be universal donors [SEE BELOW].)
- Group AB individuals will have neither anti-A nor anti-B antibodies
People with type AB blood are called universal recipients because they can receive any of the ABO types. (Actually, they need to be Rh+, too, to truly be universal recipients--that is, AB Rh- won't be happy getting any Rh+ blood [SEE BELOW].)
Universal Donors: O Rh- blood.
Universal Recipient: AB Rh+.
ABO incompatibility can cause acute hemolytic transfusion reactions. Due to strict safeguards in the health system, mismatched blood transfusions only happen 4 out of every 1 million units of blood transfused but can be very serious.
Another type of "transfusion" reaction occurs with hemolytic disease of the newborn (erythroblastosis foetalis) and organ transplant rejection.
The Rh System
Besides the ABO system, there are also important Rh antigens, which are proteins that are important to the RBC membrane. Of the >45 different Rh antigens, the most common are the:
- D,*
- C,
- c,
- E, and
- e Rh antigens.
*The commonly used terms for Rh factor--Rh positive and Rh negative--refer only to the D-antigen, but less commonly are other variants--the Rh(D) is only one variant. Rh(C), Rh(c), Rh(E), and Rh(e) exist, as does Rh-null (absence of any Rh antigens--rare).
Rh+: Rh-positive persons have RBCs with the Rh(D) antigen.
RH-: Rh-negative individuals have RBCs that do not have the Rh(D) antigen or it is deactivated.
Blood Types
Both the ABO and Rh subtypes must match if two RBC populations are to get along.
- Type A+ (type A in the ABO system with the presence of Rh(D) antibody).
- Type A- (type A in the ABO system with the absence of the Rh(D) antibody).
- Type B+ Type B-
- Type AB+ Type AB-
- Type O+ Type O-
Rh antibodies:
Just as the presence or absence of the (D) antigen is a particular blood type, the other Rh variations of antigens can also designate incompatibility with different antigenic RBCs, such as the C, c, E, and e Rh antigens.
The majority of antibodies to Rh antigens arise from exposure to blood from another individual (e.g.,, from transfusion or pregnancy).
Pregnancy
In pregnancy, the most severe incompatibility and the one that most jeopardizes an unborn baby is the Rh-incompatibility, when an Rh- mother has an Rh+ baby and their different RBC populations mix at birth with separation of the placenta. As such, this jeopardy awaits the next pregnancy. However...
Pregnancy can cause a tragic accidental transfusion reaction in a current unborn fetus, however, leading to death or severe disability. Hemolytic disease of the newborn (HDN) or hydrops fetalis (severe edema related to hemolysis) is life-threatening if not fatal.
Usually, this is a phenomenon occurring in a second pregnancy, when the mother's immune system is primed by the first and ready to strike with a subsequent pregnancy. However, it can also happen in even a first pregnancy if there is any mixing of RBCs prior to delivery via:
- Amniocentesis or chorionic villus sampling (CVS).
- Bleeding during pregnancy.
- Attempts before labor to manually turn a fetus from a breech presentation.
- Trauma to the abdomen during pregnancy.
Scenario 1: An Rh- mother has a baby with an Rh+ man and the baby is Rh+. At birth, with placental separation, there is mixing of the two different types of blood. The mother mounts an anti-Rh+ immune response to the baby's Rh+ blood she is exposed to, but the baby is safe because he or she is already born and out of the hematological picture. However, baby #2 will be the victim, trying to grow in the mom who is now primed to reject any Rh+ blood.
"There's an app for that!"
Rh- women are given an antigen called Rh-Ig (Rh Immune Globulin: RhoGAM and other brands) at the time of birth so her body will already think the response has been made and won't create the anti-Rh+ antibodies. The Rh-Ig's structure, while blocking her antibody response, is too bulky a molecule to cross the placenta in a subsequent pregnancy, so Rh-Ig doesn't jeopardize the next fetus. Everybody's happy.
If both the mother and father are Rh-, there is no need to fear an Rh-incompatibility in their baby.
Scenario 2: An Rh+ woman has an Rh- baby. Thankfully, the fetal immune system is too immature to launch an effective anti-Rh+ response at birth with the mixing of RBCs. Therefore (in girls) this lack of response means this will not sit as a time bomb for when she comes of age and were to get pregnant, probably with an Rh+ fetus.
Besides Rh-incompatibility, the fetus is not immune to ABO incompatibility, which occurs in 15% of all pregnancies. However, it only causes hemolytic disease in 4% of babies and when it does, it is much milder. They can develop hyperbilirubinemia jaundice, however.