Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Airway Obstruction
Category: Airway
Topic: Advanced Airway Management
Level: AEMT
Next Unit: Airway Suctioning
10 minute read
Airway Obstruction
The airway comes first in the ABC's because its obstruction is a quick killer that can be difficult to identify in unconscious patients. Obstruction of the airway leads to unconsciousness in seconds and death in minutes. This section will go into further depth on airway obstruction and several associated conditions.
Initial Assessment
The first step in assessing the airway is to attempt to get the patient to speak. If a patient can speak normally and there are no visualized foreign objects in the mouth the airway is clear. Unconcious or non-communicative patients require further assessment.
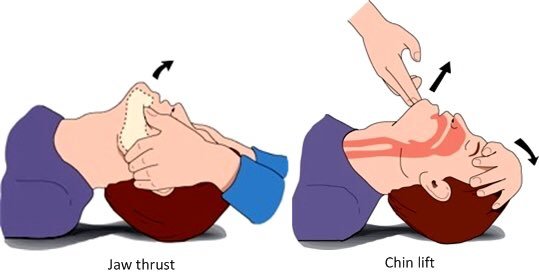 in an unconscious patient with no suspected C-spine injury, you should use the "head tilt and chin lift" technique to clear the tongue from the airway and visually inspect the pharynx for obvious foreign material, removing any material that is visualized. Patients with potential spinal injury should only be assessed using the "jaw thrust maneuver" as C-spine stability is paramount.
in an unconscious patient with no suspected C-spine injury, you should use the "head tilt and chin lift" technique to clear the tongue from the airway and visually inspect the pharynx for obvious foreign material, removing any material that is visualized. Patients with potential spinal injury should only be assessed using the "jaw thrust maneuver" as C-spine stability is paramount.
Assessing the respiratory rate, heart rate, blood oxygenation, and end-tidal CO2 (if ventilation is used) are important in the initial survey.
Categories of Obstruction
Airway obstruction is categorized into complete vs. incomplete and upper vs. lower airway obstructions.
COMPLETE OBSTRUCTIONS: A complete obstruction is the absolute occlusion of the airway that prevents any passage of air. Generally, these are caused by inhaled foreign objects. Swelling of the airway from allergic reactions or trauma can also cause an incomplete obstruction that progresses to a complete one.
INCOMPLETE OBSTRUCTIONS: Any blockage that only slows the movement of air as opposed to blocking it completely is partial. Countless things cause partial airway obstructions, the most dangerous incomplete obstructions are those that easily transition to complete ones. Trauma, allergic, infectious, and inhaled objects are some of the most alarming causes.
UPPER OBSTRUCTION: An upper obstruction is one that occurs anywhere above the vocal cords. An obstruction just above the vocal cords at the level of the larynx will not be visible by eye and will require special tools.
LOWER OBSTRUCTION: A lower obstruction is one that occurs anywhere below the vocal cords. Generally, blockages stop being called "airway obstructions" when you reach the lobes of the lung. A blockage of the lower trachea or the mainstem bronchi is still considered a proper airway obstruction.
Other Considerations in Airway Obstruction
When assessing patients with airway obstruction it is important to evaluate the work of breathing, the sounds of the upper airway, and the presence of any penetrating injuries.
WORK OF BREATHING: look for signs that the patient is working harder than usual to take a breath. The most common signs of increased WOB are retractions of the skin between the ribs, positioning the body in a tripod stance, and the inability to speak in full sentences. In pediatric patients, elevated WOB is indicated by "see-saw" breathing, strong deep breaths taken in an upright seated position where the stomach expands on inspiration and the child hunches forward on exhalation.
UPPER AIRWAY SOUNDS: it is common for the source of airway obstruction to be edema or spasm of the larynx, either due to illness or the inhalation of foreign material. This leads to an airway sound known as "stridor." Described as a harsh high-pitched whistle heard over the neck or upper chest, stridor is a strong indication that obstruction of the upper airway has occurred.
PENETRATING INJURY: A stab or shot to the face or neck places patients at extreme risk for progressive airway obstruction. Collection of blood in the spaces of the neck will collapse the trachea eventually, even when proper pressure is applied to the wound and external blood loss has stopped. An impaled object that directly blocks the airway and is leading to breathing difficulty should be removed. All other impaled objects should be left in place and stabilized. Penetrating wounds to the neck can hit the apex of the lungs and lead to tension pneumothorax.